
Retaining Medical Records
I’ve worked in HIM (Health Information Management) for over 30 years now, I started when the HIM Department was called the Medical Records Department. And retention of records has always been a burden – pretty much anyway.
I remember working in ‘the dungeon’ (record file room), didn’t every HIM department across the states have one, or still does? It was a constant battle to upkeep the file room. Organizing files and strategy planning of storing active and inactive records was a must to manage medical records.
The same principles still exist today if you still have paper medical records. Here are some of those procedures:
Creating a file folder
Assembly of the record documentation
Defining the legal record
Completion of record documentation
Filing the record
Storing the record
Purging documentation from the record
Retrieval of records
Releasing information from the record
Destroying records
Security of records
It was a yearly event to purge the dungeon in order to make room for new records and box older records for storage. It took physical strength to lift boxes of records and shuffle shelves of records. But the work involved to manually log each box of records, then create a spreadsheet of logged records was imperative if you ever needed to pull that record out of storage. I remember the agony of a misfiled record; we even had a process of how to locate a missing record.
The government mandates the retention of medical records. There are at least three regulations that must be followed – federal, state and HIPAA (Health Insurance Portability and Accountability Act). And of course, these three regulations do not match, therefore, you must follow the retention rules of whichever is more stringent. HIPAA retention regulates a minimum of 6 years, while federal retention is 7 years. And then we have state regulations. We have 50 states with varying retention regulations. This is how they tally up:

To be quite honest, I don’t know why each state would have different retention regulations. I’m sure there are good reasons for this, otherwise they would be the same, right? Or could it be that no one really pays attention to these regulations and therefore no changes or revisions are actually done. I do believe there are annual reviews by the legislature to determine if revisions are needed for state statutes. And I do believe there are hundreds of thousands of laws for possible review. Which could be the reason for no revisions to retention of medical records at the state level. I get it.
As I researched and looked up these retention regulations, it got me thinking as to why we have such a wide variation of retention years. What are the possible reasons? I’m positive there are many valid reasons out there, but shouldn’t we really have the same reason(s)?
As the medical record documents the transaction of business in healthcare, there is a few reasons it should be retained. This tells me that the medical record should be kept, for the majority of reasons, for legal purposes, for continuation of care, for provider reimbursement and, let’s not forget, quality.
There are time constraints as to filing a lawsuit for medical malpractice. On average, a person has 2 to 6 years to file a lawsuit for medical malpractice. And federal audits will not look farther back than 6 years. A retention period of 6 years minimum sounds acceptable now, right?
Medical records are used for continuation of patient care. There are times that a patient needs to change their primary care physician, or seek care from a specialty care physician, and this requires releasing copies of records for continuation of care. Having performed this task too numerous of times during my years in the HIM department, as well as networking with other HIM professionals, I found that most requests for records, on the average anyway, ask for the previous 5 years of treatment on a patient to view the patient’s medical history. A retention period of 6 years minimum sounds acceptable now too, right?
Reimbursement for medical care provided to a patient is determined by the documentation in their medical record. There is a golden rule, one might say, and that is – if it wasn’t documented, it wasn’t done. Medical records are reviewed once treatment is performed for completeness and for diagnostic and procedural code assignment. These codes then map to a bill or claim for the services provided. Payment is obtained from the patient’s healthcare insurance carrier and/or the patient. A provider normally has one year to submit a bill. Copies of medical records are released for verification of services provided as well as justification for denied claims. Therefore, a retention period of 6 years minimum sounds more than acceptable, right?
Quality – yes, let’s not forget quality purposes. Medical records are reviewed internally by healthcare providers to ensure the quality of services provided. Reviews are not only internal, but external as well. Audits of records by accrediting agencies, government and payors are normal practice for healthcare providers. The look back period for copies of medical records is between 2 to 6 years. So now, a retention period of 6 years minimum sounds acceptable, right? (you already knew I would ask that, didn’t you)
All the reasons for retention of medical records that I have mentioned here, are really the major reasons, as I do believe there can be many reasons to retain records. But so far, 6 years of retention does sound pretty good, I must say. Although, I do need to also mention another component, and that is medical records of adults compared to minors. Most states will keep minor’s medical records at least until the age of majority which is 18, and then retained at a minimum of years past 18. Again, each state has their own regulation shown in the table below.
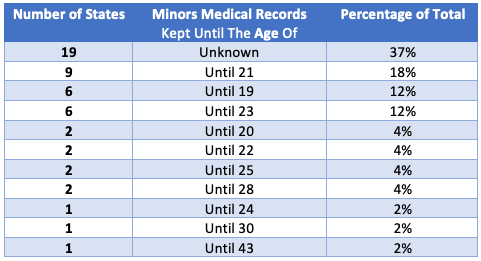
19 states did not list if they have a different length of retention, which I assume should then be the same retention as adults. But the majority of states, 29, retains records from 1 to 10 years, with the average of all those retained at 5 years past the age of 18. This leaves me to think that 6 years retention past the age of 18 sounds about right too.
Paper records have now evolved to electronic records (EMR) and have been around for over 10 years now. And electronic records have the same retention regulations as paper records. Most people would assume that retaining electronic records should be easier now – shouldn’t it? Well, an EMR must be capable of retaining a lot of data, and I mean a lot. I really think that most HIM departments don’t have a priority toward following up on electronic record retention either. I wonder if healthcare organizations actually review, purge, and destroy electronic records as stipulated by policies and regulations. Just as HIM departments maintain paper records, they should still maintain their electronic records. That should be considered best or at least standard practice to do this.
I should mention another issue of an EMR. A lot of healthcare organizations that purchased and use an EMR will change to a different EMR. And now the issue is how to access electronic records in the previous EMR – gotta love technology. IT departments are heavily used to assist HIM in transitioning records, archiving records, integrating records so that accessibility is maintained. A lot of money is used to obtain this necessary action. I would think that if retention regulations were standardized across the United States, and if healthcare organizations would comply to those regulations, it would make life in HIM easier, as well as saving a lot of dollars spent for retention that is simply a waste.
Retention of records is simply a task that is not thought of enough. A lot of healthcare organizations pay a vendor to store and maintain paper records just as they pay for a vendor to archive/store electronic records. These dollars add up and sometimes will not go away for quite a long time. HIM departments must think about this, we must be diligent in ensuring an efficient medical record. I’m not sure what steps need to be taken, not sure how to take a stab at the issue, not sure how to obtain resources on the issue either. But I do believe it is time to start the process, start to realize the issue and work toward a solution, as that solution may not show itself right now, but if we don’t start, there never will be a resolution to retention of medical records.